Typically, only see sporadic cases outside of Africa in people who have traveled to certain regions or have been in close contact with those travelers
From the 1970s up until 2003, sporadic cases were identified in central and western Africa
Before 1980, case-fatality rate was 17% and secondary transmission was the cause in 9% of cases
From 1981 to 1986, the case-fatality rate was 10% and secondary transmission was the cause in 28%
From 1996 to 1997, the largest outbreak of human monkeypox occurred, which had a case-fatality rate of 1.5% and secondary transmission was the cause in 78%
The 2003 outbreak, was the first documented cases in the western hemisphere with a case-fatality rate of 0% and secondary transmission was the cause in 0%
Cases of Monkeypox in 2022 from May 6th – 20th [2]:
UK: 20 (Confirmed)
Spain: 23 (Unconfirmed)
Portugal 5 (Confirmed) + 15 (Unconfirmed)
US 1 (Confirmed)
Precise prevalence and incidence are limited (But both have increased since the discontinuation of routine smallpox vaccination)
Wide range of hosts which has allowed a reservoir in wild animals and some sporadic cases in humans
In contrast to smallpox, monkeypox associated with low transmissibility between human beings
Mode of transmission remains poorly characterized:
Large respiratory droplets most likely mode of transmission
Direct contact through bodily fluids also possible
The likelihood of transmission between individuals without prolonged close contact is considered to be low
Hosts/Reservoirs:
Primary reservoir is thought to be squirrels, non-human primates, prairie dogs, rabbits, and rats
Primary reservoir for human infection remains unknown
Who to Suspect:
Travelers to known endemic areas
Anyone in contact with a traveler to a known area
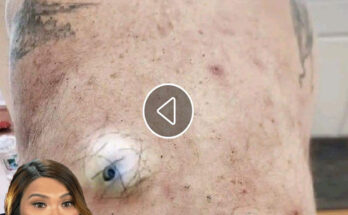
Clinical Features:
Clinically monkeypox is almost indistinguishable from smallpox, chickenpox, and other causes of vesiculopustular rashes
Typical incubation period 10 – 14 days (up to 21 days)
Infectious period occurs during the 1st week of the rash
2-day prodrome manifested by fever, malaise, and lymphadenopathy typically occurs before development of rash
Lymphadenopathy is key distinguishing characteristic of human monkeypox compared to smallpox
90% of patients infected with monkeypox develop lymphadenopathy (Typically in submandibular, cervical, postauricular, axillary, or inguinal areas)
Rash begins as maculopapular lesions of 2 to 5mm in diameter
Typically, centrifugal pattern (from the torso outwards)
Can be monomorphic (like smallpox) or pleiomorphic (like chickenpox)
Skin lesions typically progress from popular, to vesicular, to pustular, and crust phases over a 14-to-21-day period
In patients with smallpox vaccination the rash will be milder and only ≈50% will have lymphadenopathy
Most patients will not become seriously ill
In the 2003, US outbreak (81 confirmed cases) there were zero deaths [1]
Mortality seems to be higher in children, young adults, and immunocompromised individuals
Generally, cases are mild, and people tend to recover within weeks